Right Ventricle
Visual assessment of all 4 windows, but the short axis and apical 4-most important
- If RV dysfunctional may indicate volume overload
- Ventilator can cause same effect with normal RV function
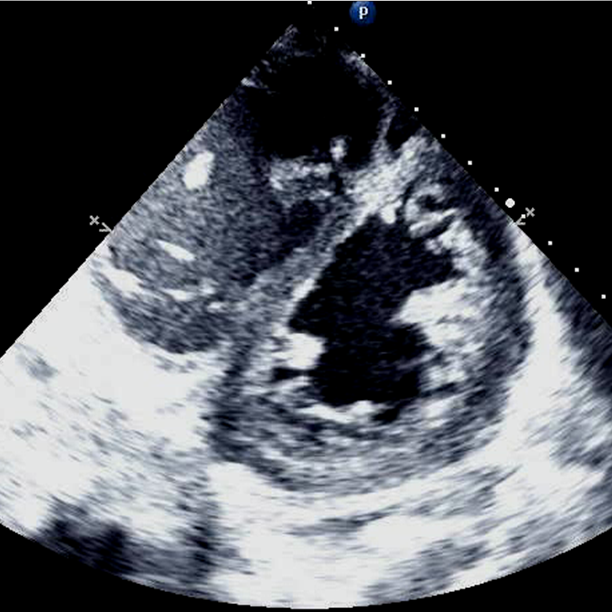
- Septal flattening and D-shaped LV
- Enlarged RV
- Best seen at the papillary level
- Enlargement of the RV relative to the LV
- The RV should be 1/3 the LV
- Maybe closer to equal in intubated patients
- Anterior motion of the RV at the tricuspid valve
- Basis of TAPSE, but can be assessed visually
Graded as normal function or mild, moderate and severe dysfunction
Do not overthink; it will become intuitive quickly
Think of it is as: Fine, not great and terrible
Make sure to use cardiac exam or presets. If using abdominal imaging the heart will look dysfunctional
If the RV is foreshortened (looks more like a softball then a football) it may look dysfunctional when function is normal
{kind=link}
{kind=link}
Clip 2 - Severe RV dysfunction, PSL View
{kind=link}
Clip 3 - RV enlargement, PSL View
{kind=link}
{kind=link}
Clip 5 - D shaped LV, PSS View
{kind=link}
{kind=link}
Clip 7 - Severe RV Dysfunction, A4C View
{kind=link}
{kind=link}