Apical 4 & 5
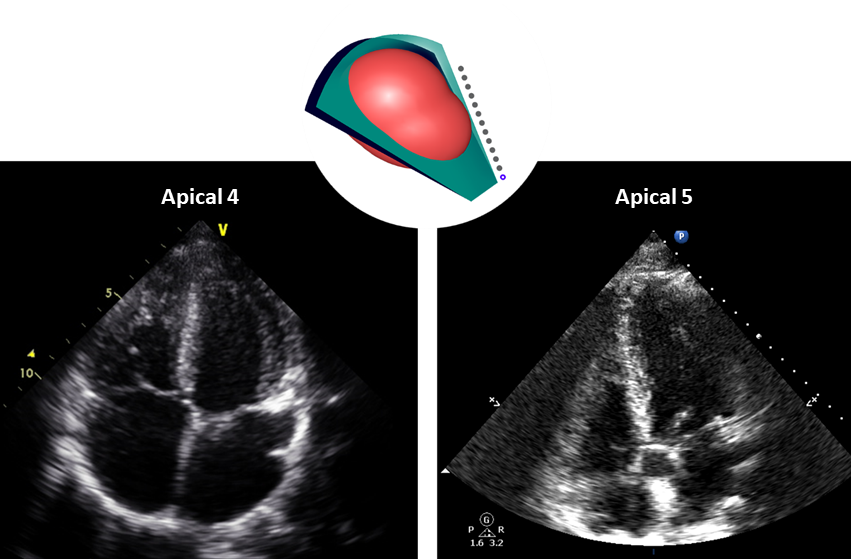
The apical 4 chamber and apical 5 (AP 4, AP 5) chamber views are high-yield images for measurements. The AP 4 is obtained first, then the transducer head is angled slightly up to open the left ventricular outflow tract (LVOT) which is referred to as the 5th chamber.
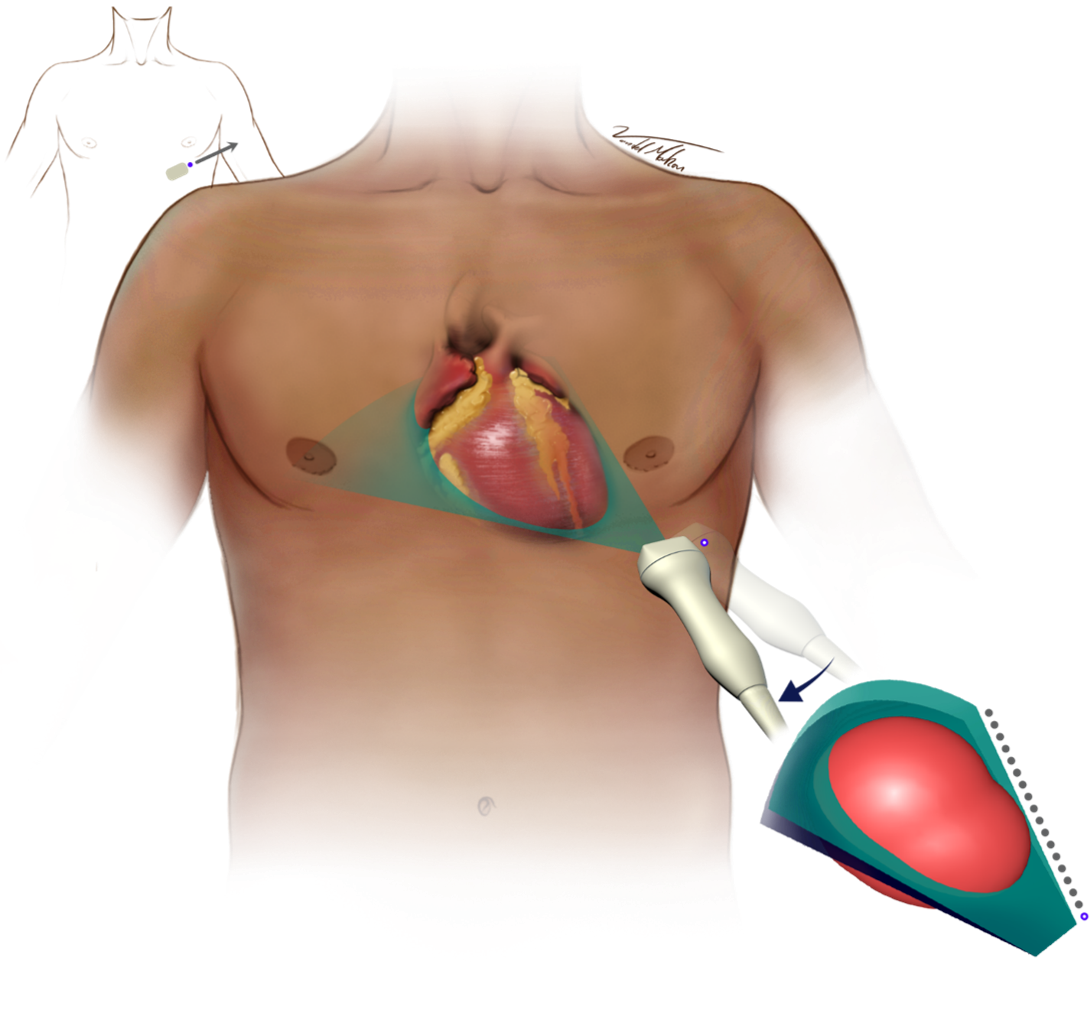
- Start lateral to the mid-clavicular line at the 4th-5th intercostal space and move medially (aim for the patient’s point of maximal impulse)
- May be more medial and lower in intubated patients
- Pendulous breast tissue, elevate the tissue and place the transducer under the breast fold
- The indicator points to the patient’s left mid-axillary line (3 o’clock position, or down towards the bed)
- From the AP 4 angle the face of the transducer opening up the left ventricular outflow tract (LVOT) to obtain the AP 5
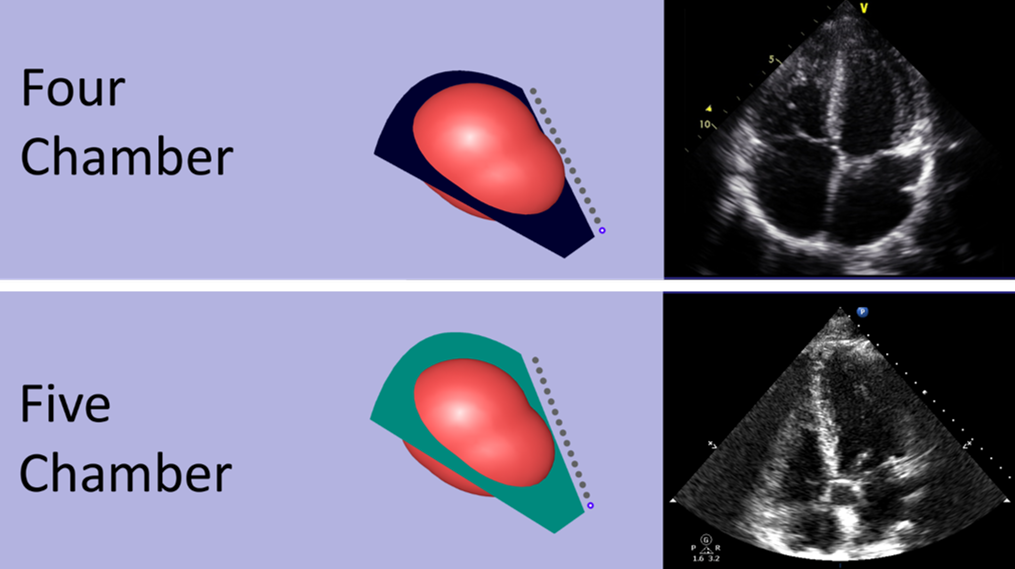
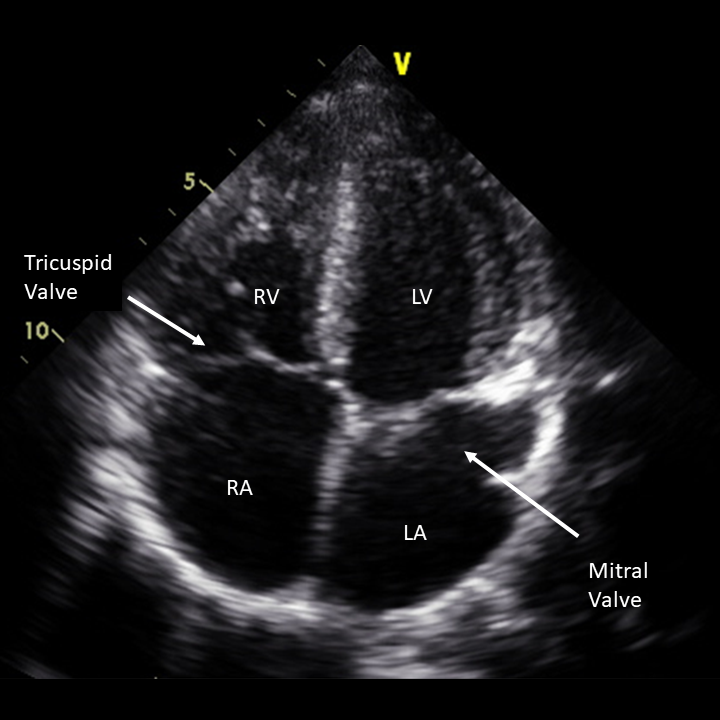
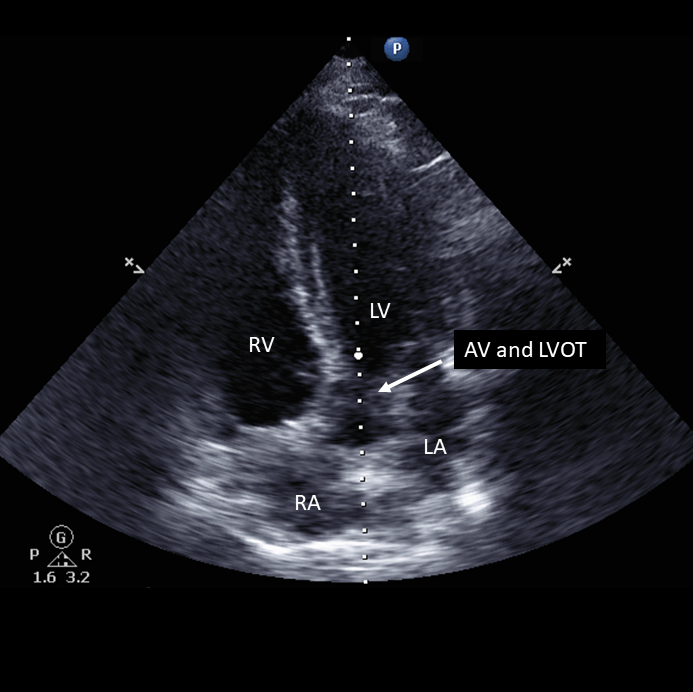
The right ventricle (RV), left ventricle (LV), left atria (LA), right atria (RA), mitral valve, tricuspid valve are well visualized
The LVOT is well visualized, the RV and LV can also be seen. The RA and LA are harder to see in this window
Measurements of diastolic function are obtained in the AP 4 and measurements of stroke volume and cardiac output are obtained from the AP 5
Figure 1 - Transducer Placement
{kind=link}
Figure 2 - Apical 4 and 5 Windows
{kind=link}
Figure 3 - Apical 4 and 5 Windows
{kind=link}
{kind=link}
{kind=link}
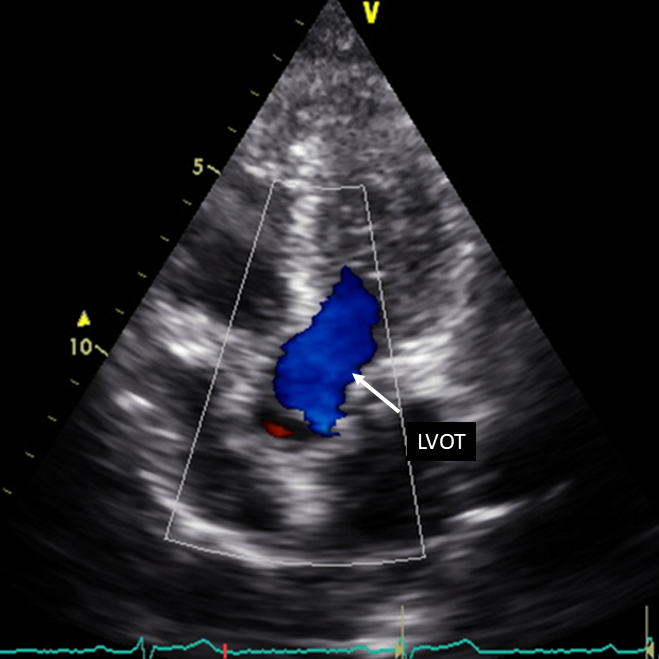
Figure 6 - Ideal A5C with color flow Doppler through the LVOT
{kind=link}
Clip 1 - A4C with Cardiac Preset
{kind=link}
{kind=link}