Hepatic Vein Flow
- Phased array probe in cardiac presets.
- Anterior axillary line with pointer towards the head.
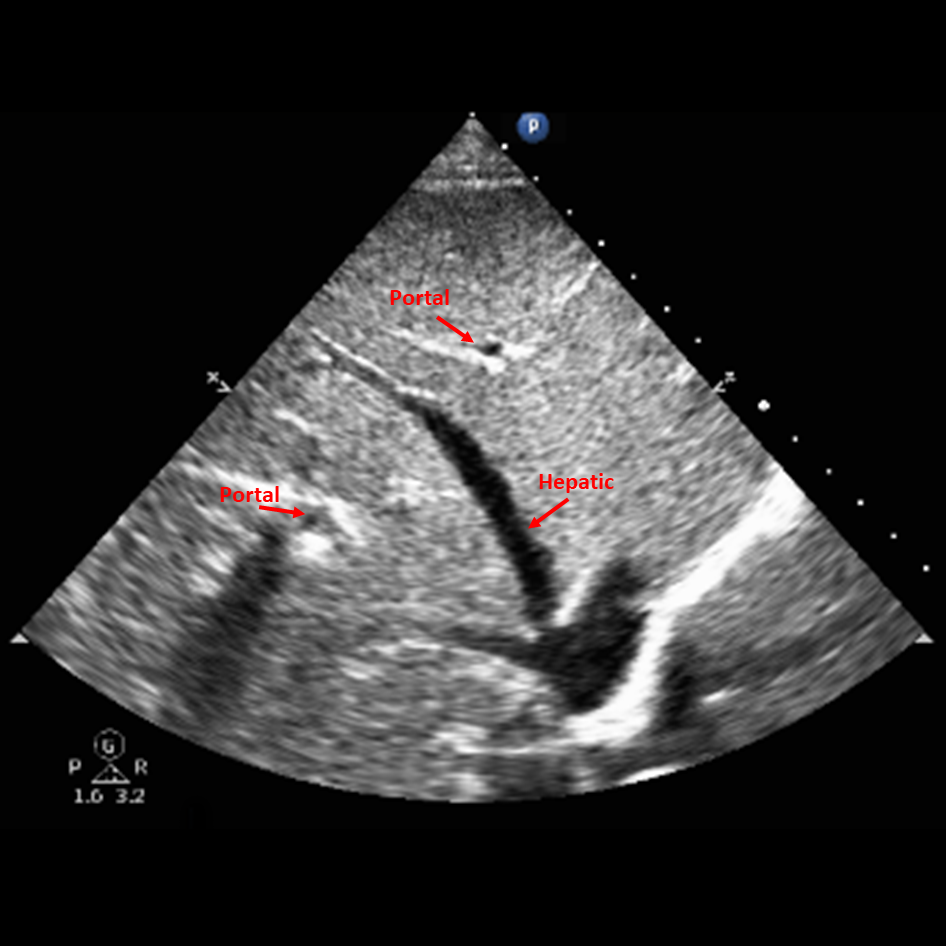
- The hepatic vein is a large hypoechoic thin walled vessel (Figure 1).
- Place EKG Leads.
- Place the color Doppler over to the hepatic vein to identify flow.
- Place the pulse wave Doppler over the hepatic vein.
- Minimize the gate.
- Acquire the PW signal and adjust the scale to optimize the waveform.
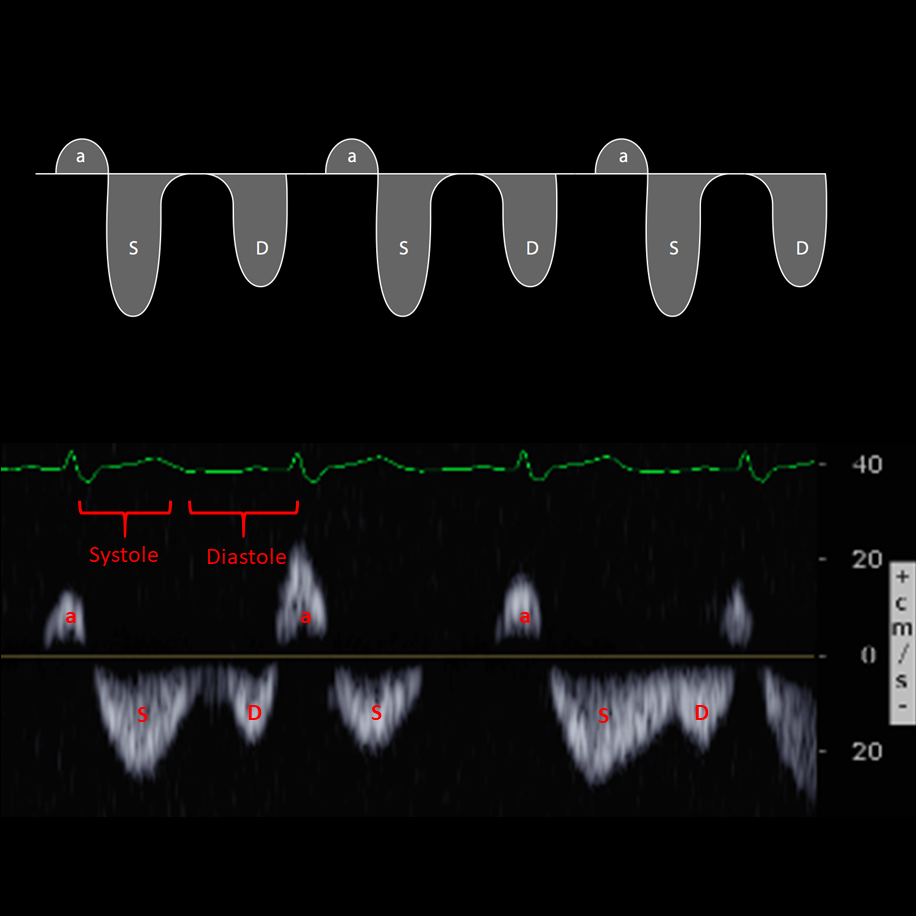
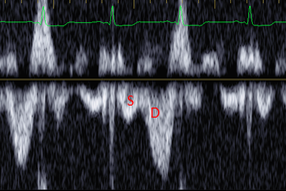
Waveform (Figure 2)
Easier with ECG
- The systolic (S) wave is first wave after the QRS.
- The diastolic wave (D) is after the (S) wave.
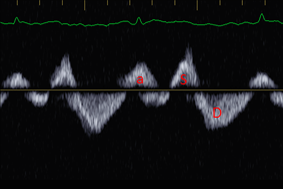
Without the ECG
- Identify the atrial (A) wave above the baseline.
- A wave can be hard to find in Afib, or with a noisy baseline.
- Identify the S after the A, and then the D after S.
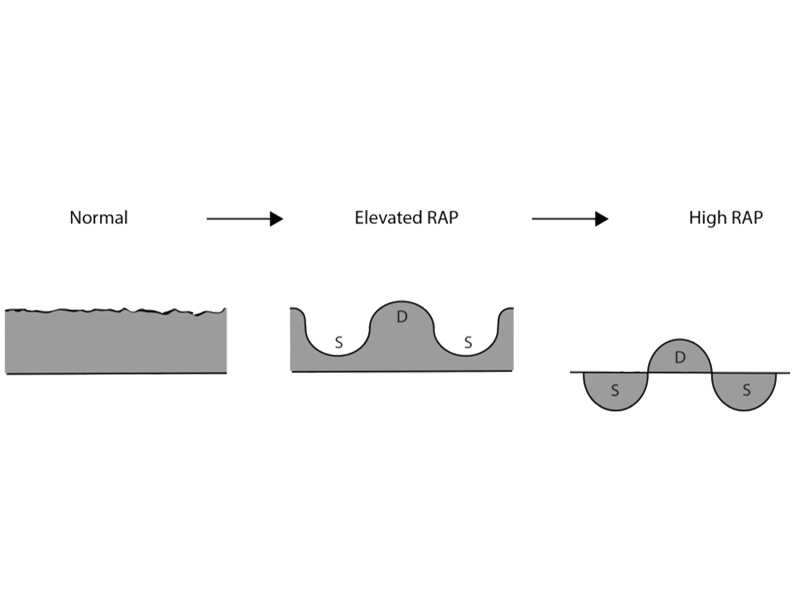
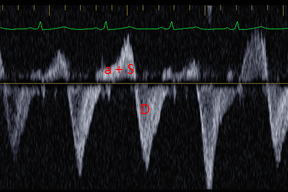
RAP and Hepatic Vein (Figure 3)
- Elevated Right Atrial Pressure (RAP).
- Normal S wave > D wave.
- Elevated S wave < D wave.
- High S wave is above the baseline and often fused with the A wave.
Hepatic Veins should be distinguished from the thick hyperechoic walled Portal Vein.
Interpretation of the waveform can be difficult.
The correlation with increased right atrial pressures should be in conjunction with other clinical and ultrasound findings.
{kind=link}
Figure 2 - Normal hepatic waveform
{kind=link}
Figure 3 - Hepatic vein waveform with increasing RAP
{kind=link}
Figure 4 - Hepatic vein waveform, normal
{kind=link}
Figure 5 - Hepatic vein waveform, S smaller than D
{kind=link}
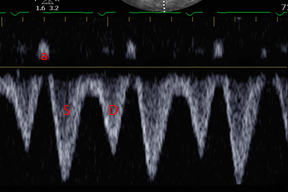
Figure 6 - Hepatic vein waveform, systolic reversal of flow
{kind=link}
Figure 7 - Hepatic vein waveform, systolic reversal of flow, A merges with S
{kind=link}
{kind=link}