FREE
FREE stands for Focused Rapid Echocardiographic Evaluation.
The FREE focuses on obtaining functional hemodynamic data to guide decision making regarding fluid management, inotropic support, and vasopressor use.
The primary indication is complex shock and respiratory Failure.
- Height, weight, HR, blood pressure
- See Education/FREE/Measurements
- Normal X 3
- Vasodialated / High-Output
- Hummingbird
- Dysfunctional
- This patient at this time
- Fluid liberal or Fluid conservative
- Based on fluid strategy and hemodynamic profiles
- Phased-array probe and a cardiac preset/exam for all imaging except lung
- Lung presets/exam for lung imaging
- If measuring hepatic venous flow apply ECG leads
- All clips should be 5 seconds or >/= 5 heart beats
Save 2D clip (Video 1)
- Assess LV function
- Assess RV function
- Look for Aortic Valve (AV) stenosis
Bonus: Save color flow Doppler (CFD) Clip
- Look for Mitral valve regurgitation
- Look for AV Insufficiency
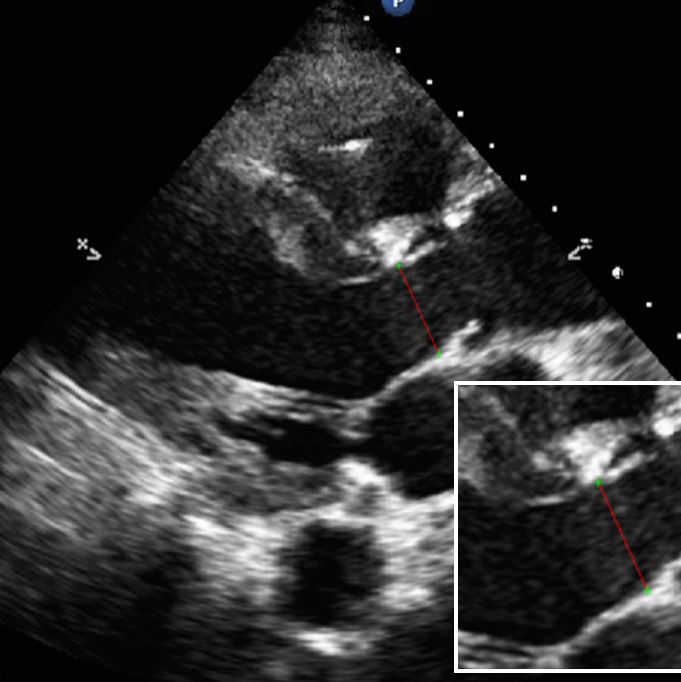
Measure/save left ventricular outflow tract diameter (LVOTD) (Figure 2)
- Used for stroke volume (SV) and cardiac output (CO)
- If unable to measure, consider modified body surface area (BSA) to estimate LVOTD
Modified Body Surface Area to estimate LVOTD
- If BSA < 1.8 M2 use 1.8 cm to estimate LVOTD
- If BSA 1.8-2.2 use BSA in cm to estimate LVOTD
- If BSA > 2.2 use 2.2 cm to estimate LVOTD
Save clip at the papillary level (Video 2)
- Assess LV function
- Assess RV function
- Look for D shaped LV
Save 2D clip Video 3
Save CFD clip
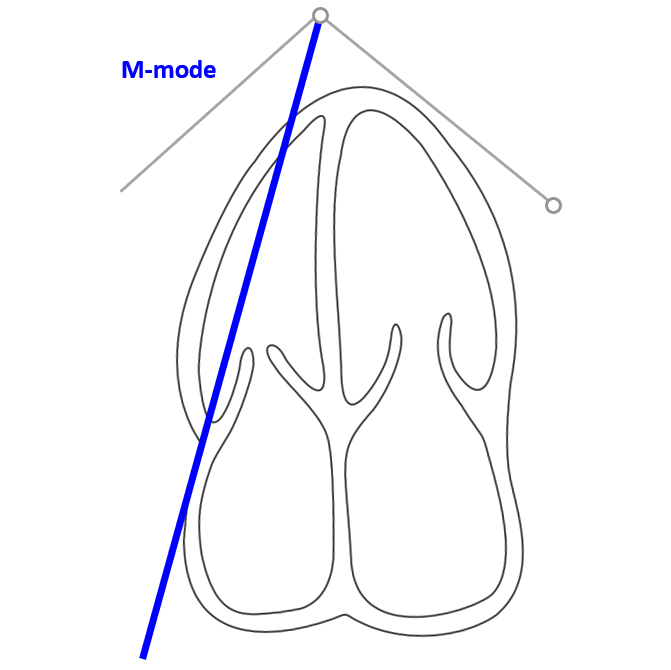
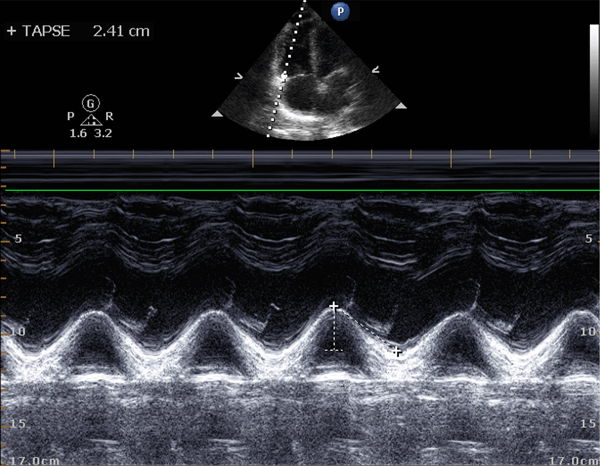
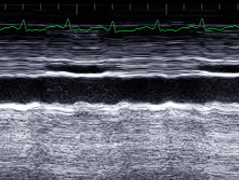
Measure/save TAPSE with M-mode (Figure 5, Figure 6)
Bonus: if concern for elevated PA pressure
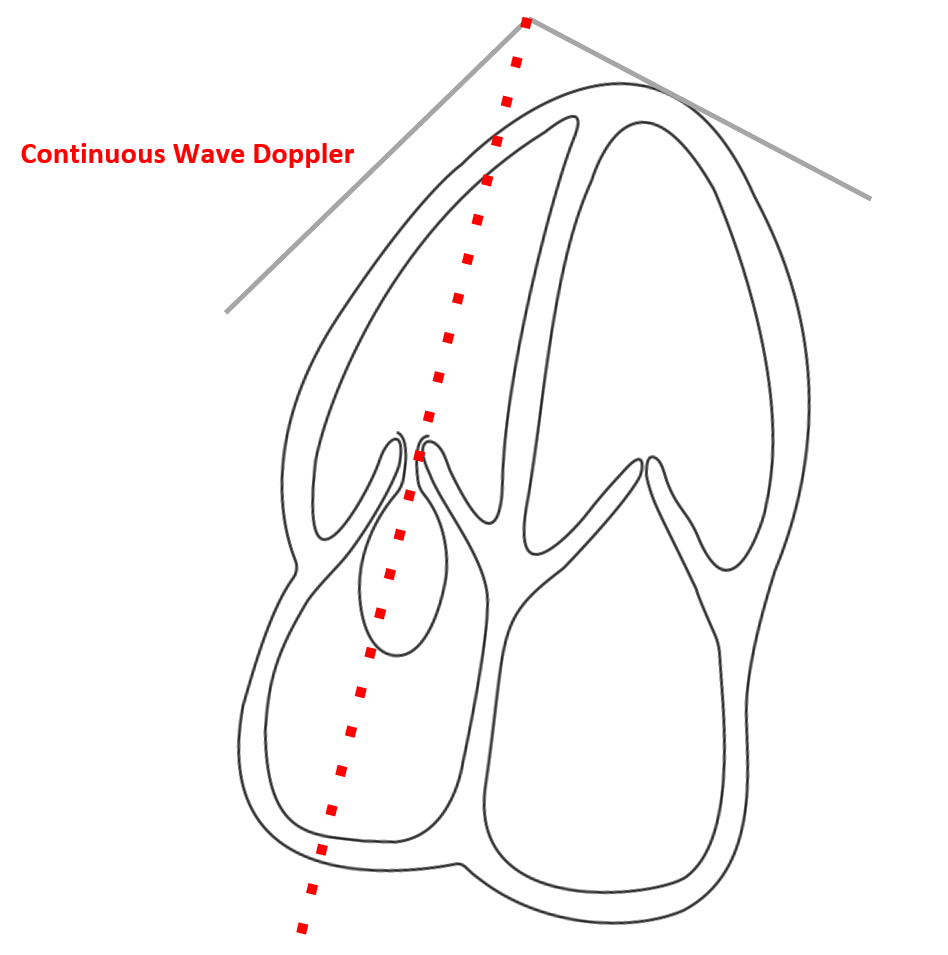
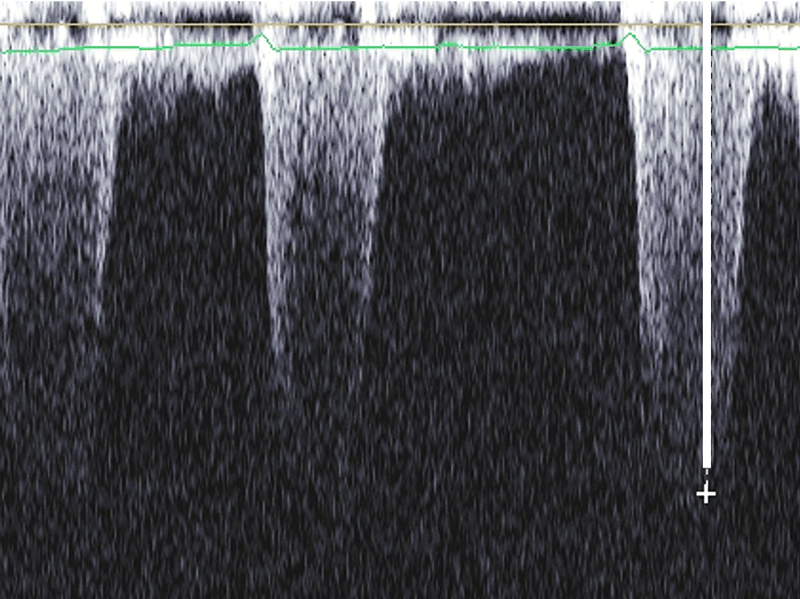
- Assess for tricuspid regurgitant jet (TRJ) (Figure 7, 8)
- Measure/save TRJ peak flow (used for estimating systolic pulmonary artery pressure )
Save 2D clip
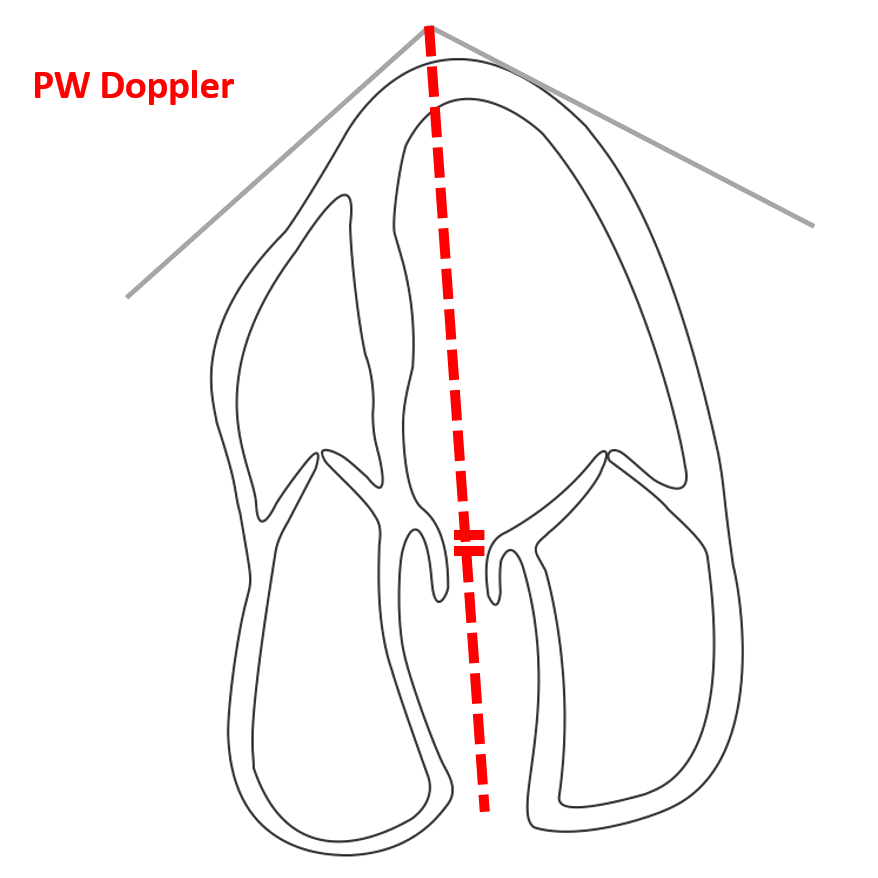
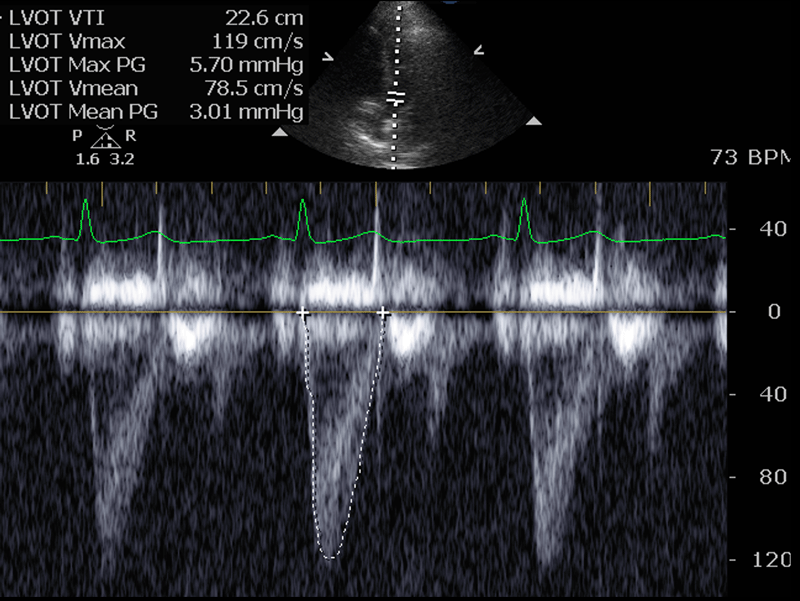
Pulsed wave Doppler through the LVOT -Measure/save the LVOT velocity time integral (VTI) (Figure 9, 10) -Used for SV/CO
Bonus: if in sinus rhythm (Figure 11, 12)
- Increase sweep speed to 75 mm/sec
- Measure peak to peak stroke volume variation
- Used for respiratory stroke volume variation (SVV)
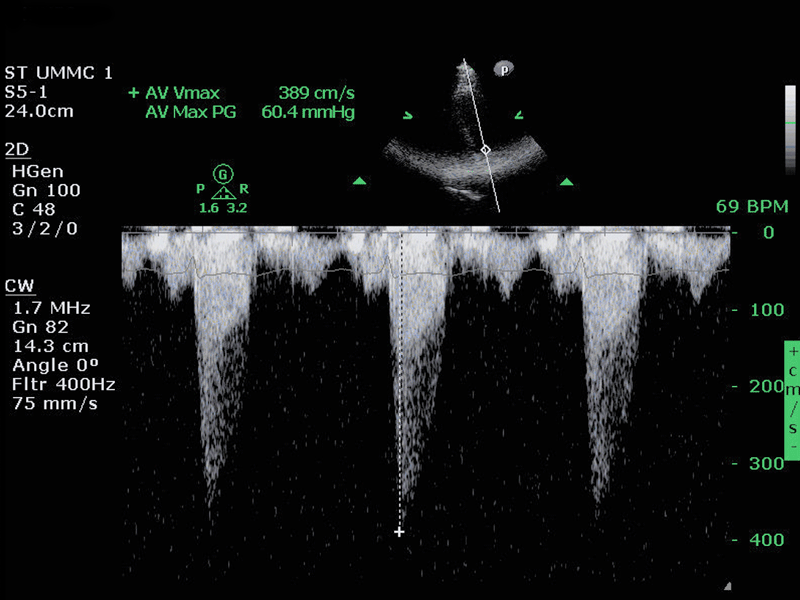
Bonus if concern for aortic stenosis (Figure 13)
- Assess/save wave Doppler through the AV
Use only if unable to assess other windows
Consider if pericardial effusion seen
Save 2D clip IVC (Video 4, Figure 14)
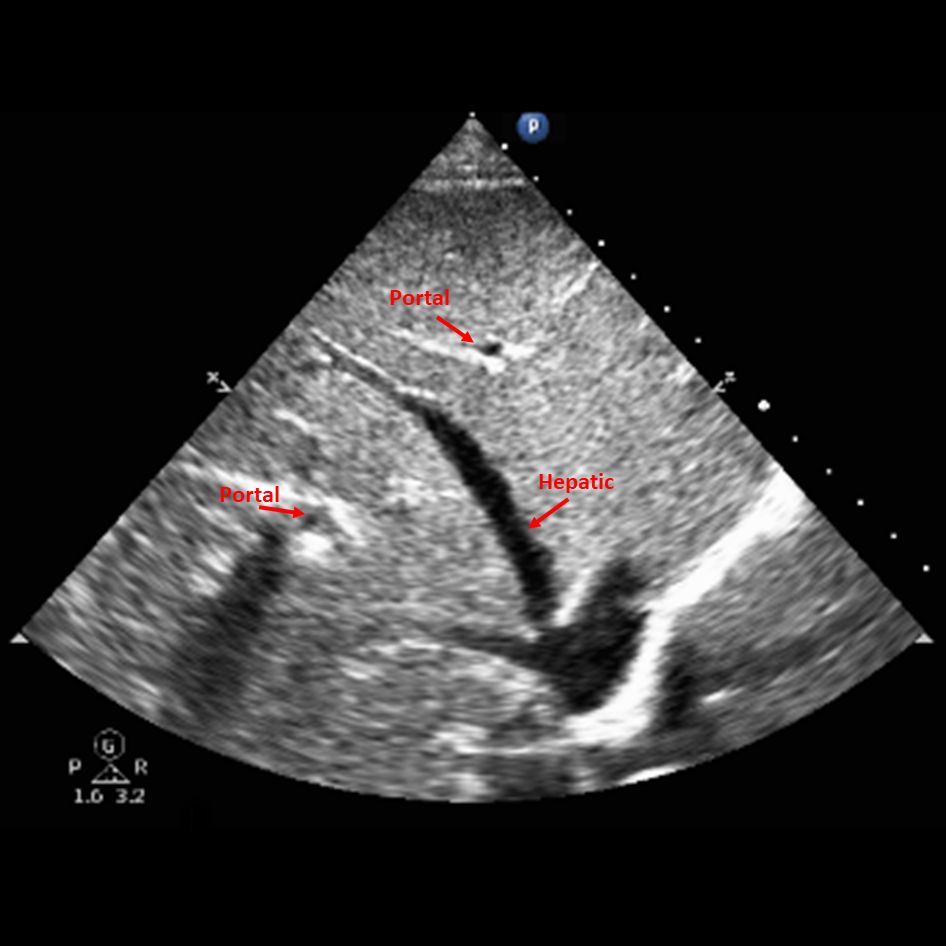
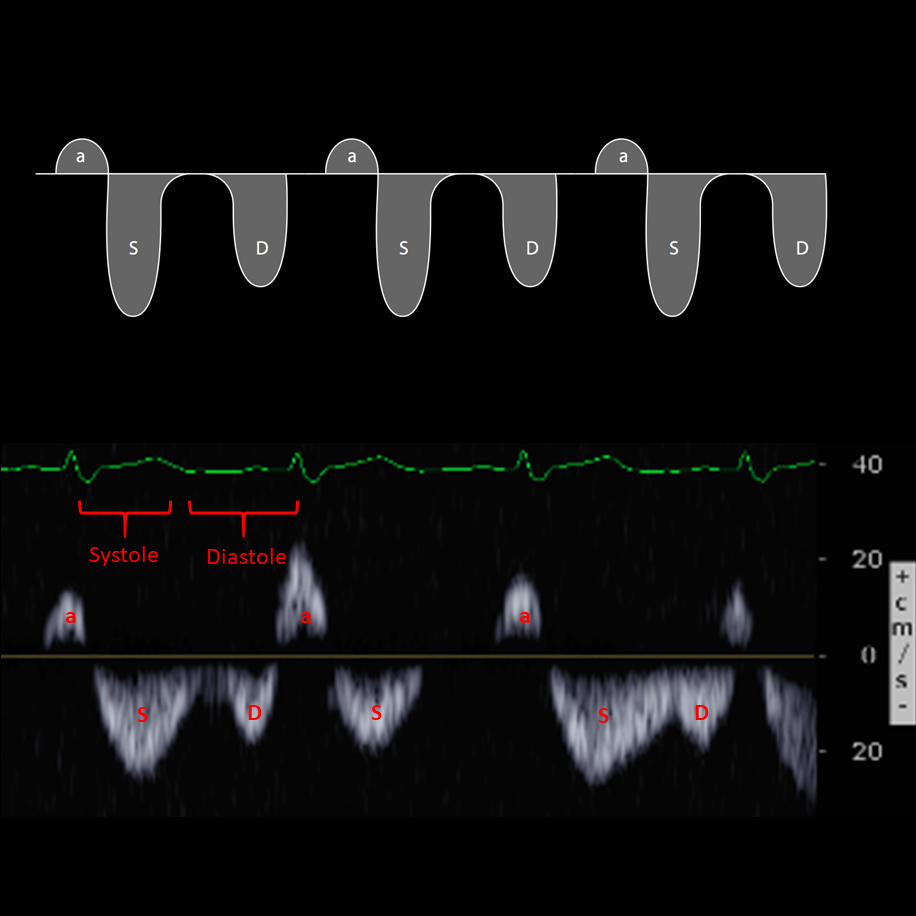
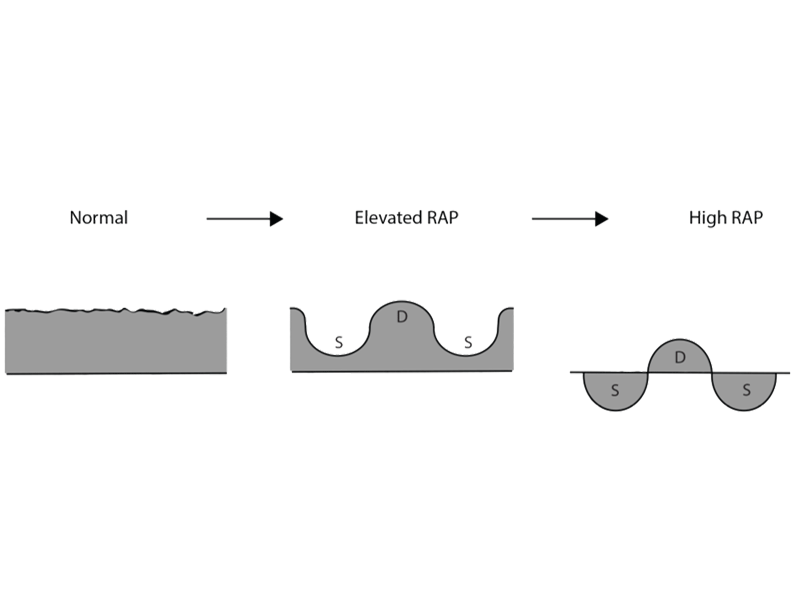
PW through hepatic vein (Figure 15, 16)
- Assess flow pattern (Figure 17)
- Used to assess for elevate right atrial pressure (RAP)
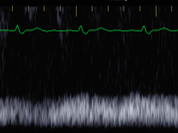
PW through a portal vein
- Assess for portal pulsatility (Figure 18)
- Used to assess for elevated RAP and portal hypertension
Change to lung or abdominal presets/exam type
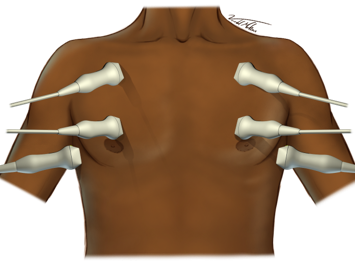
Left anterior chest upper, middle, lower (Figure 19)
Right anterior chest upper, middle, lower
- Save clips
- Assess for B-lines
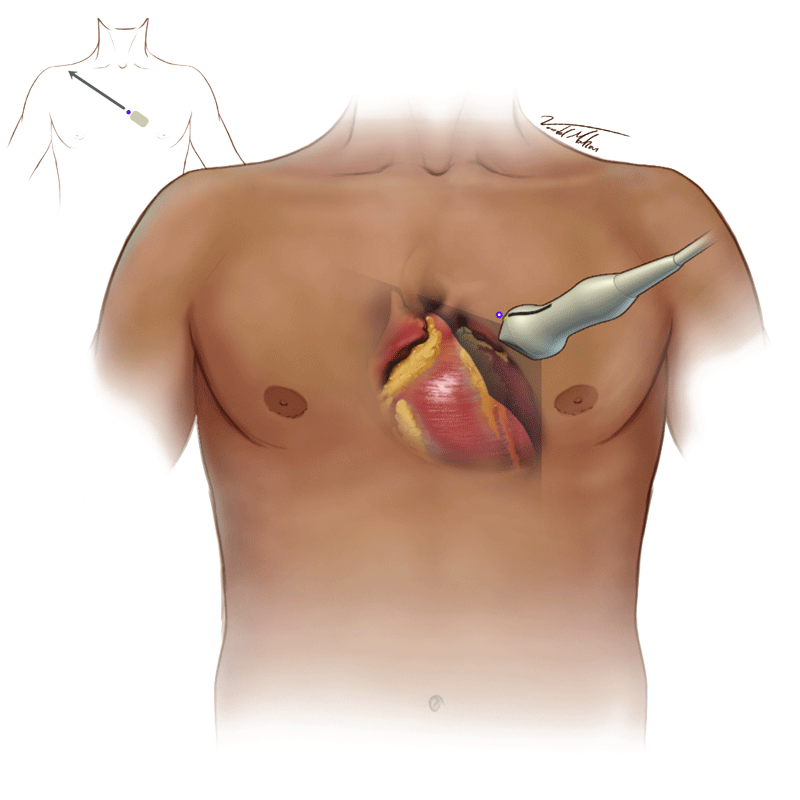
Figure 1 - Probe Placement in PLA Window
{kind=link}
Figure 2 - Measuring LVOT Diameter
{kind=link}
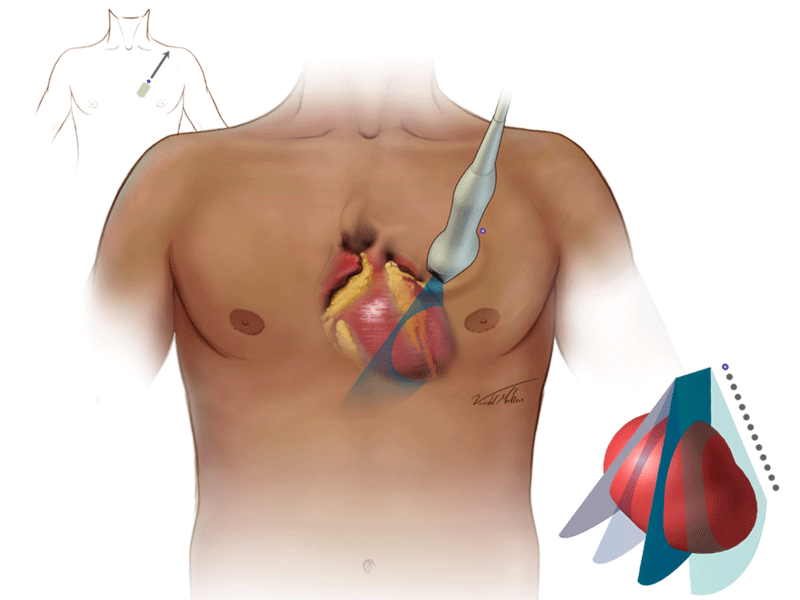
Figure 3 - Probe Placement in PSA Window
{kind=link}
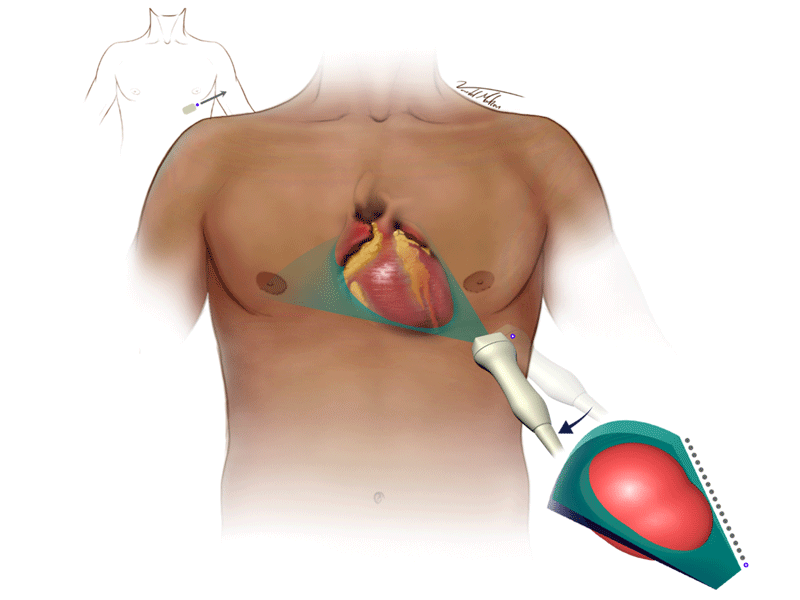
Figure 4 - Probe Placement in Apical 4 & 5 Windows
{kind=link}
Figure 5 - Apical 4 TAPSE Measurement
{kind=link}
Figure 6 - M-mode to Measure TAPSE
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 15 - Hepatic and Portal Veins
{kind=link}
Figure 16 - Hepatic flow with elevated RAP
{kind=link}
Figure 17 - Normal Portal Flow
{kind=link}
Figure 18 - Changes with elevated portal pressure
{kind=link}
Figure 19 - Transducer Placement for FREE
{kind=link}
{kind=link}
Clip 2 - PAS Window at Papillary Level
{kind=link}
{kind=link}
{kind=link}
{kind=link}