Inferior Vena Cava Variation
- Obtain a subcostal 4 chamber view using a phased array transducer in cardiac mode.
- Rotate the transducer counterclockwise aiming towards the patient’s head.
- Fan the transducer to the patient’s right (over the liver).
- The best view of the IVC shows the IVC entering the right atrium.
- use if unable to obtain subcostal view.
- Place a curvilinear transducer in abdominal mode on the mid axillary line with the probe marker towards the patient’s head.
- Aim the probe posteriorly to view the IVC passing through the liver.
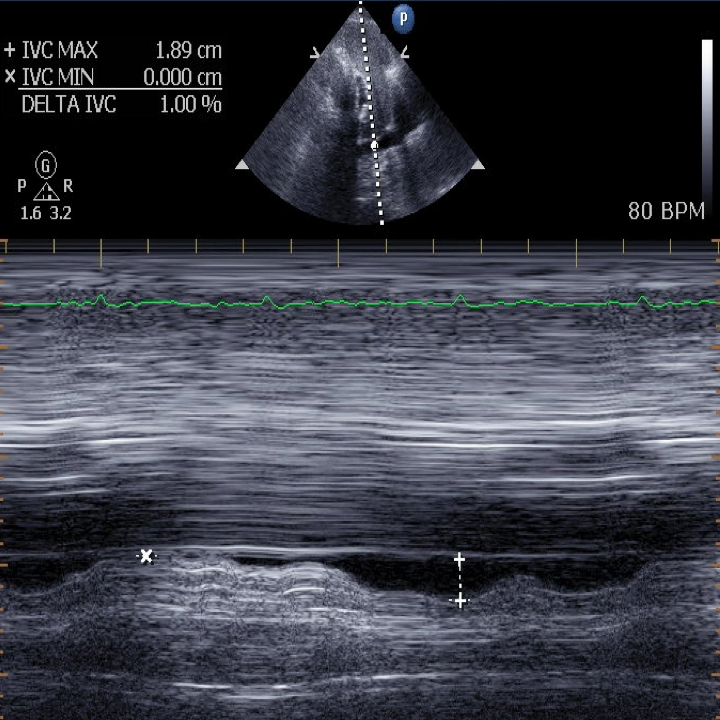
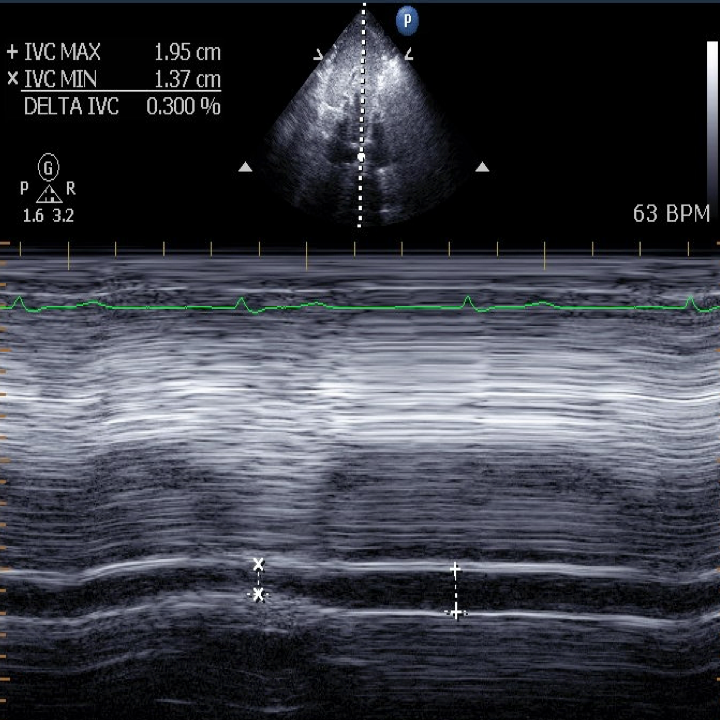
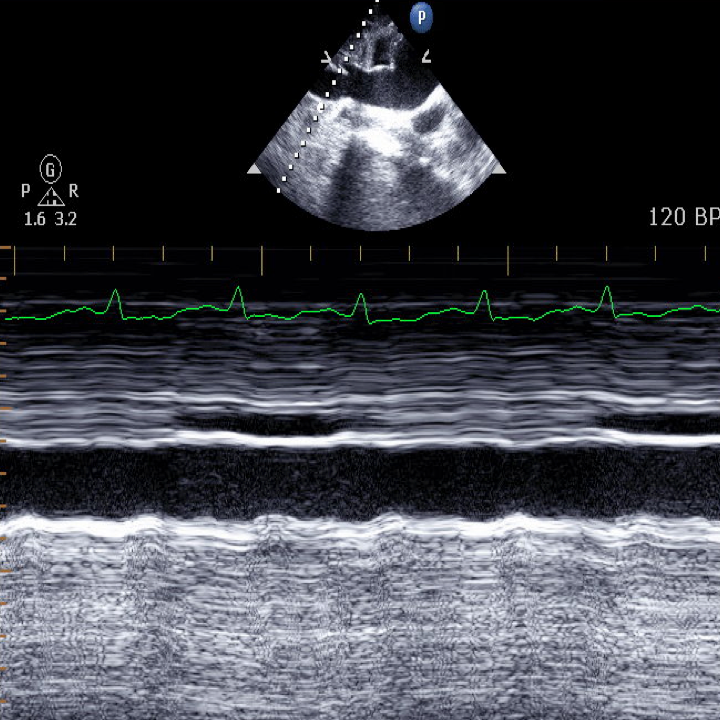
- Obtain 2D clip of IVC.
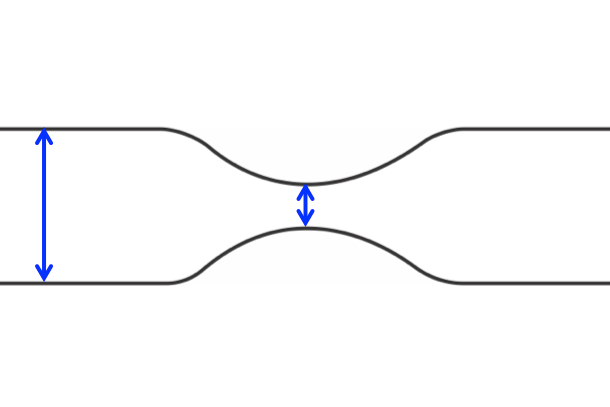
- Place the M-mode cursor through the IVC at the point of maximal variation.
- Measure the maximum IVC diameter and minimum IVC diameter .
- If IVC is angled so that the M-mode cursor is not perpendicular, use 2D image to measure variation.
Different methods with slightly different thresholds
Feissel: ΔIVC = 100 x (IVC max-IVC min) / IVC mean
Barbier: ΔIVC = 100 x (IVC max-IVC min) / IVC min
- Passively Ventilated Patients: > 18% likely volume responsive.
- Spontaneously Breathing Patients: > 25% suggests fluid responsiveness.
FREE method - Passively ventilated
- less than 10% less likely volume responsive
- 10-20% indeterminate
- more than 20% more likely volume responsive
FREE method - Spontaneously breathing
- less than 25% less likely volume responsive
- 25-50% indeterminate
- more than 50% more likely volume responsive
Can confuse aorta for IVC, make sure to see hepatic veins coming into the vessel.
IVC diameter and degree of collapse are influenced by an awake patient’s respiratory effort.
The amount of pressure support from a ventilator can impact IVC variation.
Patients with chronic lung hyperinflation, right heart failure, increased intra-abdominal pressure will have an inaccurate IVC collapsibility.
ΔIVC should be used in context with other volume measurements.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}